

[Note: This was extracted from an article written in 2010 posted on my old website: channelingreality.com]
In 1993, when for the first time in history, the first lady, Hillary Rodham Clinton attempted to become actively involved in the operation of government in a policy making capacity, it was to write legislation for a project to redesign our health care system. The lead analyst working with Hillary Clinton was Ira Magaziner. According to an article on Ira Magaziner in Slate Magazine, Bill Clinton formed the task force in the first month of his presidency (emphasis):
“First, a little history: President Clinton formed a 12-member task force in the first month of his presidency, appointed Hillary Clinton as chair, and gave them 100 days to draft new health-care legislation. Magaziner, a member of the task force, organized an “interdepartmental working group”–comprising bureaucrats and health-care experts–to supply the task force with facts and policy proposals. Magaziner divided the working group into 12 “cluster groups” and 38 “subgroups.” The number of working-group members grew from 100 to 630.”
Ira Magaziner
Ira Magaziner was a big systems designer and in my opinion, a quintessential communist central planner:
Magaziner was a noted student radical. (Wikipedia). He started a company called “Telesis” (Greek for “intelligently planned progress”). “…He started out by restructuring the curriculum of Brown University and trying to convert a small American city into a model of municipal socialism… In 1983 he volunteered the services of Telesis to help the state’s Strategic Development Commission. The result was a vast scheme, in the form of a thousand-page report called the Greenhouse Compact, to revitalize Rhode Island’s struggling economy. The name derived from a proposal to launch nonprofit research ”greenhouses” for fledgling industries.” (Fortune) Mr. Magaziner was a Rhodes Scholar at Oxford University with Bill Clinton, and his intellectual imprint is evident in Mr. Clinton’s campaign manifesto, “Putting People First. In a 1990 study called “America’s Choice: High Skills or Low Wages,” Mr. Magaziner said the nation must train workers and reorganize the workplace to meet challenges of the 21st century. As candidate and as President, Mr. Clinton has often talked about the need for “an economy of high-wage, high-skill jobs.” Mr. Magaziner and several friends went to Brockton, (MA)… for a local experiment in social democracy…In an effort to give more power to the residents of Brockton, Mr. Magaziner and his friends supported liberal candidates for local office and established a food cooperative, a weekly newspaper, a tenants’ rights organization and a nonprofit corporation to repair dilapidated housing. (NY Times)
Ira Magaziner is a member of the Advisory Committee on Digital Age Communications at the Progress and Freedom Foundation along with Dick Armey, former Republican Majority Leader of the House of Representatives and other highly placed alleged Republicans.
The Jackson Hole Group
An article in the New York Times reveals the power connections behind Ira Magaziner for the 1993 attempt at health care “reform”. The power connections were known by the name, the Jackson Hole Group.
Hillary Clinton’s Potent Brain Trust On Health Reform
By ROBIN TONER, February 28, 1993
WASHINGTON— THE CLOCK is running on the Clinton Administration’s task force on health care, which now has only two months to produce a comprehensive restructuring of a system that has resisted comprehensive restructuring for years. But Ira C. Magaziner, who is running the mammoth policy-making enterprise with First Lady Hillary Rodham Clinton, still found time last week to make the long trip to the Tetons.
There he met with a loose-knit group of experts that has become one of the most important influences in the shaping of the Clinton plan. Known as the Jackson Hole Group for the Wyoming ski town where its members meet, it has included over the past three years about 100 academics; executives from the insurance, hospital and pharmaceutical industries; physicians; representatives of business and assorted policy makers.
…The Jackson Hole Group is, at the moment, hot — the leading proponent of “managed competition,” an approach to health insurance that was embraced by President Clinton during last year’s campaign and thus moved to the center of the policy debate.
To understand the shadowy fascination of the Jackson Hole Group, one must first understand this: An exercise in policy-making that affects virtually every major constituent, interest group and business is under way in Washington, and it is largely taking place in endless meetings of working groups behind closed doors. In such a blackout, deciphering the intellectual forces at work on Mrs. Clinton and her top advisers might hint at the outcome. While Mrs. Clinton and Mr. Magaziner have marshaled more than 300 experts to assemble the health reform proposal by May 1, the Jackson Hole Group has already provided much of the basic blueprint.
…In theory, it would band employers and individuals into large cooperatives to purchase health insurance, giving small businesses and individuals the same bargaining power as big companies. On the other end, it would force doctors, hospitals and insurers to form partnerships that would compete for the cooperatives’ business, each trying to offer the highest-quality but least-expensive health plan.
The thinking is that such competition — overseen by a National Health Board establishing standards for benefit plans — would hold down medical costs yet improve health care. As for Americans currently uninsured, contributions from employers and the Government would allow them to join a cooperative.
Two of the principal advocates of managed competition are Alain C. Enthoven, a professor of economics at Stanford University, who began formulating these ideas back in the 1970’s, and Dr. Paul M. Ellwood, a pediatric neurologist from Minnesota who is widely considered a father of health maintenance organizations.
…Dr. Ellwood, who practiced medicine for 17 years, has been advising and consulting on health policy and planning for many years through the research group he founded, called InterStudy. Mr. Enthoven, a former economist with the Rand Corporation and an assistant Secretary of Defense under President Johnson, has also consulted and written extensively on health issues. Along with Lynn M. Etheredge, a Washington-based health-care consultant, those two are considered the principal architects of the Jackson Hole initiative.
Managed Competition
The essence of managed competition is captured in this paragraph from the above article:
…it would band employers and individuals into large cooperatives to purchase health insurance, giving small businesses and individuals the same bargaining power as big companies. On the other end, it would force doctors, hospitals and insurers to form partnerships that would compete for the cooperatives’ business, each trying to offer the highest-quality but least-expensive health plan.
In general, ‘managed competition’ pits providers on one side and payers on the other with patients/consumers below the line under “the market” – at the mercy of both. The obvious problem is that health care is a personal, individual thing. And the relationship between the doctor and the patient is individual. But the individual in the managed competition model has the least power in this game despite the rhetoric.
Another obvious major flaw is that Enthoven’s managed competition doesn’t address the profit orientation of the institutional, associated provider groups and insurance companies. Nobody needs the health care system when they are healthy. Once they have a health system need, the services provided become essential. In any market where services are essential and service providers are profit-making, it’s a license to steal – “your money or your life”. In this game of “health care reform”, they attempt to mask the true nature of the relationship between consumers and providers by creating the illusion of equal team power. Their objective is to corral patients (consumers of health care) into health management organizations that are theoretically responsible for “whole person” health care.
History has shown us that group providers of health care use the twin illusions of quality based on service level statistics and the image of the facilities at the macro level. Profits are increased by the degradation in the quality of care at the micro level and the “mistakes” are buried.
About a month ago (Feb. 2020), I found a 1993 video of a zombie named Jim Cooper who was the representative from Tennessee (home of Oakridge National Laboratories) speaking to the American Stock Exchange about his legislation for health care “reform”. What he was describing is a system of market-based “managed competition”. At the end of the video – at about 30 minutes in response to a question, Cooper mentions Alain Enthoven, Dr. Paul Ellwood and the Jackson Hole Group.
As you probably already know, the history of “health care reform” was that the Clinton Administration announced the program and put Hillary on the task force working with Ira Magaziner. The public was outraged at the plan and Congress responded to the revolt and washed their hands of it. It didn’t stop the project however because for what they had in mind, it would take decades to implement. Obama Care was the public rollout of the managed competition plan that was essentially the design of Enthoven and Ellwood.
Enthoven is an Economist and Systems Analyst. He could just as easily define the framework of competition for teams in a football league. It is apparent in the design of managed competition because the human element of health care was not a factor in the design of the system.
In 1993, Enthoven prepared a paper titled, “The History and Principles of Managed Competition” that was presented at a workshop sponsored by the Robert Wood Johnson Foundation. The logic of Enthoven’s ‘Managed Competition’ system is implicit. A more accurate name for it would be ‘Managed Decisions’. To read Enthoven’s paper and my analysis of it, click HERE.
The managed competition model is the foundation for the Manhattan Project of applied genomic research. It’s a system that provides behind the scenes logical triage, selection and steering of the lab rats (subscriber/patients) through the distribution of risk, allocation and subsidization of costs and prices and the access to the electronic medical record.
At this point, you should be asking – “how do you make the leap from managed competition to a Manhattan Project for applied genomic research?” To follow the trail, you should read in sequence all of my previous work – but in particular the piece titled, “Human Genome Project” beginning at the bottom of page 25, section titled, “Integrated Research and Practice”.
When I did the research for the Texas Medicaid Algorithm Project (TMAP), I found the study that was performed by the Group Health Cooperative in Northern Idaho. Their goal with the study was to contribute to the knowledge base of the TMAP project. The TMAP project was a systems project to build the knowledge base for a computerized decision support system for psychotropic drugs. The pharmaceutical companies and the state of Texas were using the Medicaid patients as lab rats. When they were discovered, they covered it up by calling it a case of Medicaid billing fraud with the pharmaceutical companies agreeing to a settlement.
Research stemming from the discovery of the Group Health Cooperative in Northern Idaho, their participation in TMAP, their connections to the Jackson Hole Group and the evolutionary changes to the U.S. health care system itself are the evidence. When I did the original research, I compiled the trail of documentation from the Group Health website. It includes links and the actual text. The links may not be active anymore, but it doesn’t matter because I captured the text of interest. You’ll notice that I’ve highlighted some words and phrases. Those highlights are important but they are probably more important to me than they will be to the reader who is looking at this subject for the first time.
Captured Populations for Medical Research
[Note: some of the links have been recovered from the internet archive. The HMORN changed their name to Health Care Systems Research Network sometime after I wrote the article in 2010. My original article has the links as they were in 2010. 12/26/2024, I tried to update the links using the internet archive. A lot of the information on the Group Health websites has been scrubbed. That’s not really surprising considering the subject matter.]
The following is from page 10 in the section titled, ‘Leading with a spirit of collaboration’:
By 1993, CHS was expanding, with grant revenue topping more than $5 million. As staff and funding grew, so did opportunities for cutting-edge collaboration. By teaming up with researchers locally, nationally, and internationally, CHS added breadth and depth to its findings, using multi-disciplinary approaches to study larger populations. Among our key partners—then and now—are the Fred Hutchinson Cancer Research Center, Veterans Affairs Puget Sound Health Care System, and several major universities, including the University of Washington (UW), Harvard University, and the University of Michigan.
This collaborative spirit reached new heights in 1996, when CHS leaders catalyzed the formation of the HMO Research Network (HMORN), a 15-member consortium of U.S. health plans with sophisticated research capabilities. Through the HMORN, CHS works with researchers nationwide to combine and study data from a diverse population more than 10 million strong. The HMORN’s hallmark project is the National Cancer Institute-funded Cancer Research Network (CRN),
HMO Research Network, Member Organizations (Read the description given for each organization).
At this point, I would ask you to remember that the objective of the ‘managed competition model’ by Ellwood and Enthoven of the Jackson Hole Group is to eliminate employer insurance by making the employer simply a facilitator for enrollment through the cooperatives so even if you have what you think is health insurance through your employer, very soon you will be in the population pool available to the HMO Research Network. This is the method for putting the entire population into the pool for a Manhattan Project for applied genetic research.
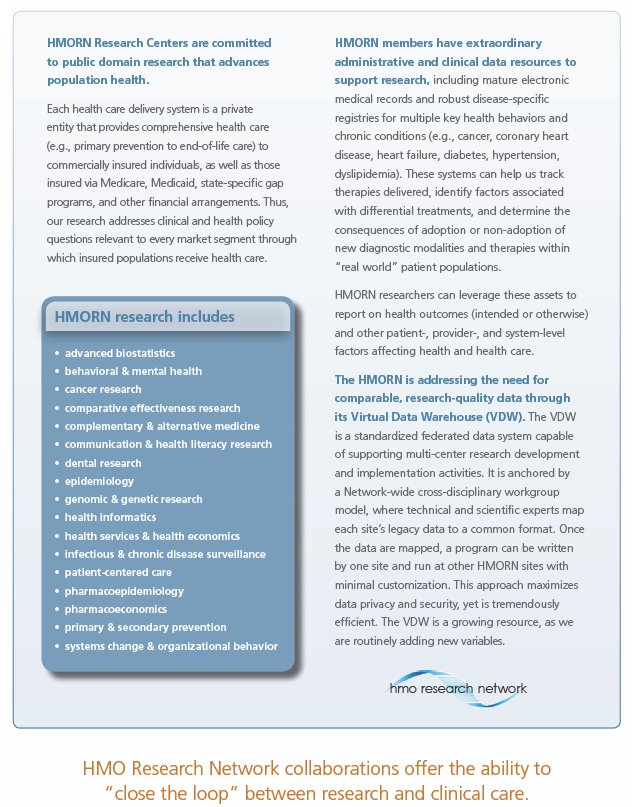
The magnitude of what they are doing is hard to wrap your head around but all of the information I’ve compiled was from information that was publicly available from their own websites. For example, I captured this description of the Cancer Research Network Virtual Data Warehouse:
VDW Boiler Plate – Short Version
So now that you know what they are doing and how they arranged the framework for it, we need to look at where the actual research and development will take place. In case it doesn’t occur to you, this system for research is uncontrollable. It’s too distributed with too many people involved – and that’s the idea. The “corridors of innovation” are the Trojan Triangles that I wrote about in 2010.
From the Bioresearch Online website article titled, 2008 International Convention’s Innovation Corridor to Highlight the Future of Biotechnology:
The BIO International Convention helps to support the association’s programs and initiatives. BIO works throughout the year to create a policy environment that enables the industry to continue to fulfill its vision of bettering the world through biotechnology innovation.
About BIO
BIO represents more than 1,200 biotechnology companies, academic institutions, state biotechnology centers and related organizations across the United States and in more than 30 other nations. BIO members are involved in the research and development of innovative healthcare, agricultural, industrial and environmental biotechnology technologies. BIO also produces the annual BIO International Convention, the world’s largest gathering of the biotechnology industry, along with industry-leading investor and partnering meetings held around the world.
The following are just a few of the biomedical research facilities that are part of the Trojan Triangle system and they aren’t even the most significant ones (universities – small business incubator system. They will use use high school, college, graduate students as “researchers”).
California LA BIOMed
Florida Biomed
Idaho – “The CORE” – biomedical research park [The CORE is the name of the Trojan Triangle referred to on the right hand side of this page]
Kansas – Biotech Corridor
Louisiana Bioinnovation Center, Pennington
Maryland HHMI
Massachusetts Whitehead, Boston Biomedical
Minnesota – Corridors of Discovery
New Jersey NJIT
Ohio “Bioinnovation Institute“, Ohio Becoming Global Hub, Northeastern universities, Knight Foundation press release
South Carolina USC
Texas – Research Valley Biocorridor
Washington State SIBCR Seattle Biomed Allen Institute for Brain Science
National Institute of Medicine Biomedical and Health Research
If you now go back to the Human Genome Project report and read it again – looking at the section on telemedicine, the Golden Parachute for doctors, the triage of patients into disease categories, the paradigm shift toward a “wellness system”, etc., you should be able to put all of the pieces together to see the strategic plan for the Manhattan Project for Real Time Biomedical Research Human Populations – applied genomics research.
And the purpose of all the above is so that when you read this page that came off the HMO Research Network website, you’ll read the words and know that they really mean what they are saying. “Words have meanings and meanings have words” and all too often today, people read things but they don’t seem to comprehend the meaning maybe because the ideas are too big or they are too horrible to contemplate.
Oh.. and btw, I didn’t just use the name ‘Manhattan Project’ just because of size and scope. I used it because the design the U.S. health care system and the plans for biomedical research are in fact, a continuation of the Manhattan Project:
Several Alta participants served either as contractors or as advisory panel members for that study. Charles DeLisi, then newly appointed director of the Office of Health and Environmental Research at DOE, read a draft of this report in October 1985, and while reading it first had the idea for a dedicated human genome project (DeLisi, 1988). The Alta meeting is thus the bridge from DOE’s traditional interest in detection of mutations to DeLisi’s push for a Human Genome Initiative, and provides one of several historical links between genome projects and another massive technical undertaking of the 20th century–the Manhattan project.
That link was obtained from this article written by Jacqueline Stevens: Tech Flesh 9: The Secret History of Jesse Gelsinger’s Death. (which I couldn’t find again). Here is a link to the CTheory website. 12/26/2024
Death Exposes Risks of Gene Therapy about Jesse Gelsinger and his death.
The Arizona teenager is the first person to die as a direct result of gene therapy, the medical revolution-in-waiting which promises to cure scores of incurable diseases but has yet to cure one.

Michael Porter, Mr. Cluster
Clusters are “geographic concentrations of interconnected companies, specialised suppliers, service providers, firms in related industries, and associated institutions (for example universities, standard agencies, and trade associations) in particular fields that compete but also cooperate”. He also points out: “a cluster is a form of network that occurs within a geographic location, in which the proximity of firms and institutions ensures certain forms of commonality and increases the frequency and impact of interactions”
Greenhouse Model of Socialism
Trojan Triangle is the name I gave to the municipal socialist organizational structure being implemented in Meridian, Idaho. At the time, I didn’t know what it was, but I did know that it was not American in the traditional conception of America. The Trojan Triangle article was my first attempt at trying to identify and define the elements of the system they were implementing. The descriptions I found of the Greenhouse Compact sounded very much like what I was seeing in Meridian.
Greenhouse Compact
1984 “A Shattered Greenhouse“ (emphasis added) “The Greenhouse promised high wage job-creation; business incentives to explore new products and markets; research facilities (the “greenhouses”) to stimulate avant-garde industrial activity in such fields as robotics and thin-film materials technology; and much more.”
1986 “Greenhouse: Why a good plan failed“ (his opinion) An analysis of the election data, collected by randomized telephone interviews within 24 hours of the referendum, revealed that the plan encountered fatal voter mistrust based on the planning process rather than the plan.
1993 “Washington at Work; An Idealist’s New Task: To Revamp Health Care“ “Recalling the referendum, Prof. George H. Borts of Brown, who describes himself as a freemarket economist, said, “Ira’s economic ideas were primitive, just off the wall.” He maintained that Mr. Magaziner seemed to assume that Rhode Island, the nation’s smallest state, could develop its own economy and thrive on exports.”
 Alain C. Enthoven was one of McNamara’s Defense Department “Whiz Kids” who was involved in the project of redesigning the Defense Department systems. In 1971, he along with K. Wayne Smith produced a book about the experience of applying Systems Analysis techniques to the process of organization and management of military and defense assets and processes. The title of the book is How Much is Enough? Shaping the Defense Program, 1961-1969
Alain C. Enthoven was one of McNamara’s Defense Department “Whiz Kids” who was involved in the project of redesigning the Defense Department systems. In 1971, he along with K. Wayne Smith produced a book about the experience of applying Systems Analysis techniques to the process of organization and management of military and defense assets and processes. The title of the book is How Much is Enough? Shaping the Defense Program, 1961-1969
Harvard Health Policy Forum for New Legislators (1992)
Alain Enthoven speaker (27:40) and Harvard’s Reincarnated Hitler, Robert J. Blendon

Dr. Paul M. Ellwood
“He wants their medical records”
Excerpt from 1988 Fortune Magazine Article, Medical Care’s Next Revolution (emphasis added):
”Half of what the medical profession does is of unverified effectiveness,” asserts Dr. Paul M. Ellwood Jr. of Minneapolis, in a phalanx of physicians who want to cut down on the guesswork. Half of something as stupendous as the U.S. health bill — now 11.4% of GNP, or nearly twice what the military gets — implies a huge ore body that could be mined for savings. That should be of special interest to business, which picks up the biggest chunk of medical expenditures . . . ”What HMOs haven’t done, which I had hoped, is manage the content of medical care,” Ellwood says. Why not? ”HMO doctors are ignorant, just like all doctors.” Having shaken up the medical system once, Ellwood seeks to do it again. He wants the records of millions of encounters between doctor and patient, whether in HMOs or in the traditional fee-for-service system, recorded in computers and the results of treatment routinely monitored
Human Genome Project Information
1990-2003
Oak Ridge National Laboratories
Oak Ridge, Tennessee





{kind=link}